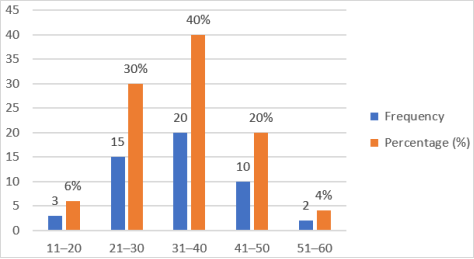
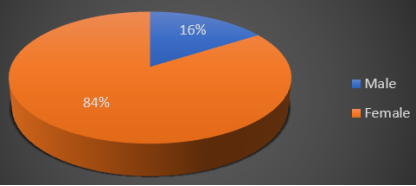
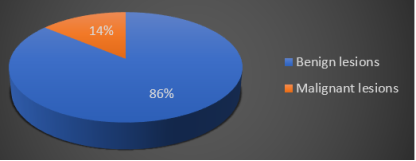
Background: Thyroid swelling is a common clinical problem and may arise from benign or malignant conditions. Although most thyroid swellings are benign, a significant proportion may harbor malignancy, requiring timely diagnosis and appropriate surgical management. Objective: To evaluate the patterns of presentation and surgical management of thyroid swellings with suspected malignancy. Methods: This observational cross-sectional study was conducted in the Department of ENT and Head neck- surgery, Rajshahi Medical College Hospital, Rajshahi, Bangladesh from June 2014 to December 2014. A total of 50 patients with clinically and ultrasonographically diagnosed thyroid swelling who subsequently underwent thyroidectomy were included. Detailed history, clinical examination, thyroid function tests, ultrasonography, Fine Needle Aspiration Cytology (FNAC), and histopathological examination were performed. Data were analyzed using descriptive statistics. Results: The age of the patients ranged from 11 to 59 years, with the highest frequency in the 31–40 years age group (40%). Females predominated (84%), with a female to male ratio of 5.25: 1. Neck swelling was present in all patients, while dysphagia (8%), pain (6%), and dyspnoea (2%) were less common. Multinodular goitre was the most frequent type of thyroid swelling (68%), followed by solitary nodular goitre (30%). Ultrasonography revealed solid nodules in 70% cases. FNAC showed colloid goitre in 76% cases. Histopathology confirmed benign lesions in 86% and malignant lesions in 14% cases. Papillary carcinoma was the commonest malignancy (85.71%). Hemithyroidectomy was the most common surgery (60%). Conclusion: Most thyroid swellings were benign; however, a considerable proportion were malignant. Careful preoperative evaluation and appropriate surgical management are essential for early diagnosis and better outcomes.
| Published in | International Journal of Otorhinolaryngology (Volume 12, Issue 1) |
| DOI | 10.11648/j.ijo.20261201.16 |
| Page(s) | 31-39 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Thyroid Swelling, Goitre, Thyroid Malignancy, FNAC, Thyroidectomy, Papillary Carcinoma
Variable | Frequency | Percentage (%) |
|---|---|---|
Symptoms | ||
Neck swelling | 50 | 100 |
Pain | 3 | 6 |
Dysphagia | 4 | 8 |
Dyspnoea | 1 | 2 |
Voice change | 0 | 0 |
Cervical lymphadenopathy | 1 | 2 |
Duration of symptoms | ||
6 months–2 years | 24 | 48 |
2–4 years | 16 | 32 |
4–6 years | 6 | 12 |
6–8 years | 2 | 4 |
8–10 years | 2 | 4 |
Variable | Category | Number of Cases | Percentage (%) |
|---|---|---|---|
Type of Swelling | Solitary nodular goitre | 15 | 30 |
Multinodular goitre | 34 | 68 | |
Diffuse goitre | 1 | 2 | |
USG Findings | Solid nodule | 35 | 70 |
Cystic nodule | 15 | 30 |
FNAC Diagnosis | Number of Cases | Percentage (%) |
|---|---|---|
Colloid goitre | 38 | 76 |
Follicular neoplasm | 6 | 12 |
Papillary carcinoma | 6 | 12 |
Medullary carcinoma | 0 | 0 |
Anaplastic carcinoma | 0 | 0 |
Malignant Histological Type (n=7) | Number | Percentage (%) |
|---|---|---|
Papillary carcinoma | 6 | 85.71 |
Follicular carcinoma | 1 | 14.29 |
Variable | Total Cases | Malignant Cases | Percentage (%) |
|---|---|---|---|
Male | 8 | 2 | 25 |
Female | 42 | 5 | 11.9 |
11–20 years | 3 | 1 | 33.33 |
21–30 years | 15 | 3 | 20 |
31–40 years | 20 | 2 | 10 |
41–50 years | 10 | 0 | 0 |
51–60 years | 2 | 1 | 50 |
Type of Surgery | Benign Cases | Malignant Cases | Total | Percentage (%) |
|---|---|---|---|---|
Hemithyroidectomy | 30 | 0 | 30 | 60 |
Subtotal thyroidectomy | 8 | 0 | 8 | 16 |
Total thyroidectomy | 5 | 6 | 11 | 22 |
Total thyroidectomy with neck dissection | 0 | 1 | 1 | 2 |
FNAC | Fine Needle Aspiration Cytology |
USG | Ultrasonography |
ENT | Ear, Nose and Throat |
CT | Computed Tomography |
SPSS | Statistical Package for Social Science |
WHO | World Health Organization |
ICCIDD | International Council for Control of Iodine Deficiency Disorders |
IDD | Iodine Deficiency Disorder |
BSMMU | Bangabandhu Sheikh Mujib Medical University |
IPGM&R | Institute of Post Graduate Medicine and Research |
| [1] | Moosa FA, Junaid M, Khan FW et al. prevalence of malignancy in resected specimen of patients operated for benign nodular goitre, Pakistan Journal of Surgery. 2007; 23(2): 129-132. |
| [2] | International council for control of Iodine deficiency disorder (ICCIDD). IDD news letter 1996; 12: 1-3. |
| [3] | Sharma D, Sharma N, Sharma P, Promal R. Incidence of thyroid malignancy among goirous thyroid swellings in Rajasthan. 2014; 3(2): 1727-1733. |
| [4] | Sidhom S, Alaa M, Salah M Askary EE. General Surgery dept. Faculty of Medicine, Zagazig university. Incidence of Malignancy in Thyroid swellings. Z. U. M. 2012; 18(9): 880. |
| [5] | Htwe TT, Hamdi M, Swethadri G. K. Wong Jol, Soe MM, Abdullah MS. Incidence of malignancy among Goitrous thyroid lesions from the sarawak General Hospital. Singapore Med J 2009; 50(7): 724-728. |
| [6] | Htwe TT, thyroid malignancy among goitrous thyroid lesions: a review of hospital based studies in Malaysia and Myanmar. Singapore Med J 2012; 53(3): 159-169. |
| [7] | Riccabona G. Thyriid cancer and endemic goiter. In: Stanbury JB, Hatzel BS, eds. Endemic Goiter and Endemic Cretinism. New Your: John Wiley and Sons, 1980; 333-50. |
| [8] | Tarrar AM, Madiha D, Ilyas S. Solitary thyroid nodule; Frequency of amlignancy at combined military hospital Rawalpindi. Proffetional Med J 2010; 17(4): 598-602. |
| [9] | Shaheen OH, The thyroid gland. In scott-Browns otolaryngology, Laryngology & Head & Neck surgery, 6th edition: Reed educational and professional publishing Ltd.-1997; Page 18/1-24. |
| [10] | John M Chaplin, NEIL Sharma and John C Watkinson; Surgical Management of differentiated thyroid cancer. Stell and maran’s textbook of head neck surgery and oncology. Hodder and stoughton ltd.-2012: 5th edition: c-3, p-422-452. |
| [11] | Ramsben J and watkinson JC, Thyroid Cancer. In Scott-Brown’s Otolaryngology Head and neck surgery. 7th edition; Edward Arnold Ltd.-2008; p-2663-2701. |
| [12] | Williams NS Christopher J. K; The thyroid and The parathyroid gland. Bailey & Love’s short practice of surgery 26th edition; c-51; CRP press Ltd.-2013; p-741-776. |
| [13] | Mackenzie E and Mortimen RH. MJA Practice essentials endocrinology. Thyriod Nodules and thyroid cancer. 2004; 180: 246. |
| [14] | Mazumder et. al, Management of Thyroid Cancer: A Brief Review of Selected Literature, July 2005, Vol. 05, No. 01, P-33-37. |
| [15] | Huque et. al, Histopathological pattern of malignancy in solitary thyroid nodule, Bangladesh J Otorhinolaryngol 2012; 18(1): 5-10. |
| [16] | Rain AJH, Charles VM. The thyroid gland and the thyroglossal tract. Bailey and love's short practice of surgery, Twenty third ed: ELBS, 2000; 707-33. |
| [17] | Miller JM. Evalution of thyroid nodules. Surg Clin N. Am, 1985; 69(5): 1063-76. |
| [18] | IslamR, Ekramudduala AFM, Allam C, Kabir MS, Hssain D. Frequency and pattern of mallignancy in solitary thyroid nodule. Bangladesh J of Otolaryngology; 2009; 15(1): 1-5. |
| [19] | Hard JD. The thyroid gland. Hardy's text book of surgery, First edition: JB Lippincott Company, 1983; 371-93. |
| [20] | Browse NL. The thyroid gland. An introduction to the symptoms and signs of surgical disease, Third edition: London ELBS, 1998; 266-8. |
| [21] | Harmo J, Calrk OH. Significance of lymph node metastasis in differentiated thyroid cancer. AMJ, 1978; 136: 107-12. |
| [22] | Kendel LW, London RE. Prediction of malignancy in a solitary thyroid nodule. Lancet, 1969; 1: 1071-3. |
| [23] | Cady B, Sedgwick CE, Meissner WA et al. Risk factor analysis in differentiated thyroid cancer. Cancer, 1979; 10(6): 230-7. |
| [24] | Stark DD, Clark OH, Gooding GAW, Moss AA. High resolution ultrasonography and computed tomography of thyroid lesions in patients with hyperparathyroidism. Surgery, 1983; 94: 245-52. |
| [25] | Ashcraft MW, Van Herle AJ. Managment of thyroid nodule. Head and Neck surgery, 1981; 3: 216-97. |
| [26] | Block MA, Dailey GE, Robb JA. Thyroid nodule indeterminate by needle biopsy. Am J Surg, 1983; 20: 113-203. |
| [27] | Chandanwale S et al. Research article: Clinicopathological correlation of thyroid nodules. Int J Pharm Biomed Sci 2012; 3(3), 97-102. |
| [28] | Basharat R, HossainM, Saeed S, Hamid T. Comparison of fine needle aspiration cytology and thyroid scan in solitary thyroid nodule. SAGE-Hindawai Access to Research Pathology Research International 2011; 9. |
| [29] | Hussain N, Anwar M, Nadia N. Pettern of surgically treated thyroid disease in karachi. Biomedica, 2005; vol. 21. |
| [30] | Khairy GA. Solitary thyroid nodule: the risk of cancer and the extent of surgical therapy. East African medical journal; 2004; 81(9), 459-461. |
| [31] | Islam MS, Siddiquee BH, Akter N. Comperative study of FNAC and histopathologicaly in the diagnosis of thyroid swelling. Bangladesh J Otorhinolaryngol 2010; 16(1): 35-43. |
APA Style
Hasan, M. K., Shishi, R. A., Uddin, S., Forhad, R. (2026). Patterns of Presentation and Surgical Management of Thyroid Swellings with Suspected Malignancy. International Journal of Otorhinolaryngology, 12(1), 31-39. https://doi.org/10.11648/j.ijo.20261201.16
ACS Style
Hasan, M. K.; Shishi, R. A.; Uddin, S.; Forhad, R. Patterns of Presentation and Surgical Management of Thyroid Swellings with Suspected Malignancy. Int. J. Otorhinolaryngol. 2026, 12(1), 31-39. doi: 10.11648/j.ijo.20261201.16
@article{10.11648/j.ijo.20261201.16,
author = {Muhammad Kamrul Hasan and Rifat Anwar Shishi and Shihab Uddin and Rizvan Forhad},
title = {Patterns of Presentation and Surgical Management of Thyroid Swellings with Suspected Malignancy},
journal = {International Journal of Otorhinolaryngology},
volume = {12},
number = {1},
pages = {31-39},
doi = {10.11648/j.ijo.20261201.16},
url = {https://doi.org/10.11648/j.ijo.20261201.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20261201.16},
abstract = {Background: Thyroid swelling is a common clinical problem and may arise from benign or malignant conditions. Although most thyroid swellings are benign, a significant proportion may harbor malignancy, requiring timely diagnosis and appropriate surgical management. Objective: To evaluate the patterns of presentation and surgical management of thyroid swellings with suspected malignancy. Methods: This observational cross-sectional study was conducted in the Department of ENT and Head neck- surgery, Rajshahi Medical College Hospital, Rajshahi, Bangladesh from June 2014 to December 2014. A total of 50 patients with clinically and ultrasonographically diagnosed thyroid swelling who subsequently underwent thyroidectomy were included. Detailed history, clinical examination, thyroid function tests, ultrasonography, Fine Needle Aspiration Cytology (FNAC), and histopathological examination were performed. Data were analyzed using descriptive statistics. Results: The age of the patients ranged from 11 to 59 years, with the highest frequency in the 31–40 years age group (40%). Females predominated (84%), with a female to male ratio of 5.25: 1. Neck swelling was present in all patients, while dysphagia (8%), pain (6%), and dyspnoea (2%) were less common. Multinodular goitre was the most frequent type of thyroid swelling (68%), followed by solitary nodular goitre (30%). Ultrasonography revealed solid nodules in 70% cases. FNAC showed colloid goitre in 76% cases. Histopathology confirmed benign lesions in 86% and malignant lesions in 14% cases. Papillary carcinoma was the commonest malignancy (85.71%). Hemithyroidectomy was the most common surgery (60%). Conclusion: Most thyroid swellings were benign; however, a considerable proportion were malignant. Careful preoperative evaluation and appropriate surgical management are essential for early diagnosis and better outcomes.},
year = {2026}
}
TY - JOUR T1 - Patterns of Presentation and Surgical Management of Thyroid Swellings with Suspected Malignancy AU - Muhammad Kamrul Hasan AU - Rifat Anwar Shishi AU - Shihab Uddin AU - Rizvan Forhad Y1 - 2026/05/19 PY - 2026 N1 - https://doi.org/10.11648/j.ijo.20261201.16 DO - 10.11648/j.ijo.20261201.16 T2 - International Journal of Otorhinolaryngology JF - International Journal of Otorhinolaryngology JO - International Journal of Otorhinolaryngology SP - 31 EP - 39 PB - Science Publishing Group SN - 2472-2413 UR - https://doi.org/10.11648/j.ijo.20261201.16 AB - Background: Thyroid swelling is a common clinical problem and may arise from benign or malignant conditions. Although most thyroid swellings are benign, a significant proportion may harbor malignancy, requiring timely diagnosis and appropriate surgical management. Objective: To evaluate the patterns of presentation and surgical management of thyroid swellings with suspected malignancy. Methods: This observational cross-sectional study was conducted in the Department of ENT and Head neck- surgery, Rajshahi Medical College Hospital, Rajshahi, Bangladesh from June 2014 to December 2014. A total of 50 patients with clinically and ultrasonographically diagnosed thyroid swelling who subsequently underwent thyroidectomy were included. Detailed history, clinical examination, thyroid function tests, ultrasonography, Fine Needle Aspiration Cytology (FNAC), and histopathological examination were performed. Data were analyzed using descriptive statistics. Results: The age of the patients ranged from 11 to 59 years, with the highest frequency in the 31–40 years age group (40%). Females predominated (84%), with a female to male ratio of 5.25: 1. Neck swelling was present in all patients, while dysphagia (8%), pain (6%), and dyspnoea (2%) were less common. Multinodular goitre was the most frequent type of thyroid swelling (68%), followed by solitary nodular goitre (30%). Ultrasonography revealed solid nodules in 70% cases. FNAC showed colloid goitre in 76% cases. Histopathology confirmed benign lesions in 86% and malignant lesions in 14% cases. Papillary carcinoma was the commonest malignancy (85.71%). Hemithyroidectomy was the most common surgery (60%). Conclusion: Most thyroid swellings were benign; however, a considerable proportion were malignant. Careful preoperative evaluation and appropriate surgical management are essential for early diagnosis and better outcomes. VL - 12 IS - 1 ER -
Department of ENT, Jamalpur Medical College, Jamalpur, Bangladesh
Department of Otolaryngology, Bangladesh Medical University, Dhaka, Bangladesh
Department of ENT & Head-Neck Surgery, Mymensingh Medical College Hospital, Mymensingh, Bangladesh
Department of Otolaryngology–Head Neck Surgery, Kumudini Women's Medical College and Hospital, Mirzapur, Bangladesh
Information